
It’s interesting how to see how different countries handle the COVID-19 pandemic response. In Asia, virtually everybody is now wearing a face mask, sometimes hand-made due to supply issues, but in Europe and North America at least, I’ve seen authorities tell healthy people not to wear a mask at all, and reserve them to health professionals. I’ve even seen some nasty comments on Twitter complaining about people wearing masks at the grocery store (in the US) as they took supply out of health professionals.
I personally think this is madness for a disease that is known to transmit from asymptomatic people, and I’m shocked to learn some people working at supermarkets are not given masks. But when I send photos from Thailand to my brother in France, he’s always surprised to see everybody wearing a mask. But everything points to masks being effective.
N95 masks are the best, followed by surgical masks, but hand-made masks, or even wearing a bandana helps, although they do not filter droplets just as well, and while you wear any of those masks, you should probably just take the same precautions as if you didn’t wear any.
Governments have stockpiles of oil and food, but most (all?) did not prepare for a pandemic and face masks are in short supply. So with China having stabilized, many companies are now producing face masks, even electronics manufacturers since prices have gone through the roof, and I’m receiving emails daily about TV boxes or electronics company selling face masks… For reference, a box of 50 face masks used to cost about $2 locally, but now the quote I get for similar masks from China is closer to $14.
Some companies are also trying to help makers specifically, and for example, Seeed Studio offered free face masks to Makerspaces and Fablabs. Full disclosure: I also received a box of 50 face masks.

Sadly, all boxes are gone, but Pine64 is now giving away 50,000 face masks to makers as Pine64 factory is also making those like everybody else.
Since demand is likely to be high, priority will be given in the following order:
- Forums and chat moderators
- Partner-project developers
- Community developers (anyone who contributed code to a PINE64 device
- Developers from key projects to PINE64 community (e.g. SUNXI, Lima, Panfrost, etc.,)
- Others at my discretion
You’ll find the full details in Pine64 Forum announcement. I’ll post other face mask giveaways in the comments section if any.

Jean-Luc started CNX Software in 2010 as a part-time endeavor, before quitting his job as a software engineering manager, and starting to write daily news, and reviews full time later in 2011.
Support CNX Software! Donate via cryptocurrencies, become a Patron on Patreon, or purchase goods on Amazon or Aliexpress. We also use affiliate links in articles to earn commissions if you make a purchase after clicking on those links.


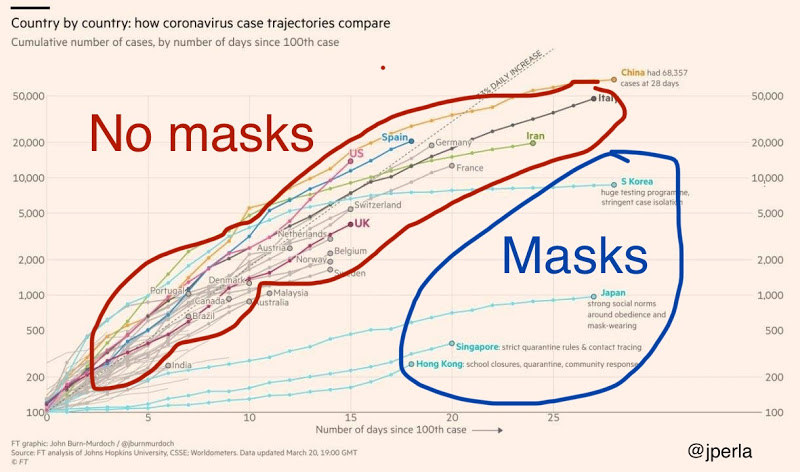
In my opinion masks are not the solution and it’s even visible on the graph. They are useful to protect people exposed to a lot of other people (doctors, supermarket workers for example), but for the rest of the population they only slow down the virus diffusion but will not prevent it from reaching 60% of the population which is the threshold above which it will stop spreading that fast, so it will just take longer and make the trouble last much longer, putting the world at stop for that long. It is absurd to think that we’ll kill this virus, it never happened in history and will not happen. Even cholera and ebola still exist and are closely watched. We can only hope to develop defenses, like for most viruses. We should aim at seeing the virus spread as fast as hospitals can reasonably deal with it without being overloaded so that we get over with that problem quickly. At the moment people are dying at home from heart attacks or brain attacks because people are scared to go to the hospital as they fear being infected! Some are suffering from their teeth and cannot find a dentist anymore! The world turned back to middle age in a few weeks and most people have become extremely selfish and spend time watching how their neighbor lives or aggressing doctors to steal their masks, it’s really pathetic.
> At the moment people are dying at home from heart attacks or brain attacks because people are scared to go to the hospital as they fear being infected!
They also die because nurses flee due to closing borders and other repressions: https://swprs.org/a-swiss-doctor-on-covid-19/#latest (and even if they later die caused by dehydration they then count as Covid19 victims and add to the death toll further increasing panic/repressions).
I find this common train of thought baffling… you can’t argue the virus can’t be contained when they’ve literally stopped the virus in Taiwan Korea and China. We’ve stopped SARS and MERS before. Yes it might flare up in very small incidents, but when the numbers are sufficiently low then it doesn’t affect the vast majority of society, health authorities can quickly respond and track down all contacts and quarantine suspects and life goes on as normal. There is no need to have a 60% infection rate.. that’s just nuts and would involved so many needless deaths. This whole thing is solvable as long as people don’t just throw up their hands and say it’s impossible. Everyone wearing masks and minimizing contact with strangers in at-risk areas is part of the solution
> you can’t argue the virus can’t be contained when they’ve literally stopped the virus in Taiwan Korea and China
This means nothing. As long as the population is not immune and there still exists at least one infected person in the world, nobody’s safe. Should we keep 7 billion people in their home-jails for years ? And should we put them in their home-jails for 3 months every year with the regular flu? At some point the paranoia must stop! People are going totally crazy, some threatening cops to spit on them, others shouting at people walking in the street! Some people have not opened their window for 2 weeks in fear that they’ll let the virus enter, and as a result they’ll get many other issues. And I’m not even counting the number of kids victim of home accidents!
@Willy It’s like you didn’t read half of what I wrote…
Life in Hong Kong/Taiwan/South-Korea (and starting in China) is not “crazy” or as hysterical as you are making it out to be. People are not under house arrest and things are more or less back to normal. I don’t know where you live, but maybe you’re projecting your current predicament onto places that have already dealt with the virus? There are minor outbreaks (due to travel) – as you say that’s kinda inevitable – but the numbers are small enough that they can be managed on a case by case basis. Yes large gatherings have been cancelled and there have been some minor life style adjustments but on the whole it’s not so different from before (this is first hand)
> Life in Hong Kong/Taiwan/South-Korea …. People are not under house arrest and things are more or less back to normal.
As it is in Sweden for example. No repressions, no excess mortality. And BTW no masks.
It might take a while until we realize that this whole pandemic is mostly a data literacy issue…
Right all the people dieing in Wuhan/Lombardy is just a statistical fluke and a product of our overly active imaginations
> Right all the people dieing in Wuhan/Lombardy is just a statistical fluke
No, but the attribution based on a newly released virus test developed in January might be. Wrt to air pollution northern Italy is Europe’s Wuhan, the health system is one of the worst and collapses regularly in Winter and the excess mortality of past Flu seasons was way higher than in other European regions (BTW: currently excess mortality is just slightly higher mostly due to local effects like medical personell in quarantine or at home looking for their children while in the rest of Europe it’s lower than in past winters).
What’s different is that now we try to look for one single virus with a test and if the dead person is test-positive we count this as Covid19 death. We deal so even with persons who showed no Covid19 symptoms at all and even so if the mortality profile corresponds closely to natural mortality (in Italy close to zero for children and almost twice as high for 75-year-old men as for women of the same age, this describes both ‘Covid19 mortality’ as well as natural mortality).
Why do we do this? Why do we give credit to a virus based on a single virus-test result if a 95 year old person dies of cancer? The average age of the positively-tested deceased in Italy is currently about 81 years. 10% of the deceased are over 90 years old. 90% of the deceased are over 70 years old. 80% of the deceased had suffered from two or more chronic diseases. 50% of the deceased had suffered from three or more chronic diseases.. Why do we treat these as killed by a new ‘killer virus’?
Correcting statistical mistakes is important and I’m sure that the misattribution of the cause of death is a problem but it’s a bit of a leap to then conclude that the horrors happening in hospitals in Lombardy and Wuhan were actually a normal seasonal occurrence that simply no one had bothered to film/document before.
I don’t take issue with your statistics, but you’re again arguing about mortality figures while the original question is if this virus is stoppable. I think evidence shows that it is. If, China, an underdeveloped country caught off-guard can stop it – then there is no reason the west can’t.
The alternative you and Willy condone is to having 60% of people sick, shrugging and letting the old/sick die and hospitalizing hundreds of thousands of young people (b/c note that while survival rates are high hospitalization rates are also not low). Not only is it quite heartless/callous but I just don’t feel it’s warranted
And ofcourse even if some countries do decide to take this radical “solution”, they will effectively be cut off from the countries that actually dealt with the issue head-on. Grandpa-killing viruses aren’t exactly shrugged off in Asia
> while the original question is if this virus is stoppable
Well, I ask myself the question whether the virus has not already widely spread. How should we know if tests are not done on a representative sample?
> having 60% of people sick, shrugging and letting the old/sick die and hospitalizing hundreds of thousands of young people
Which data is backing this? Surveys where testing not just focused on ‘sick’ or dead people in hospitals but also included asymptotic people (so going towards a representative sample) ‘found that 50% of all test-positive persons showed „no symptoms“ at all, while the other 50% mostly showed „very moderate cold-like symptoms“. According to the Icelandic data, the mortality rate of Covid19 is in the per mille range, i.e. in the flu range or below. Of the two test-positive deaths, one was „a tourist with unusual symptoms“’
So why do we treat a positive test result as illness? It might be just an infection but the tests used seem to have a high false-positive rate anyway.
BTW: I’m not suggesting anything, I simply started to ask (myself) questions last weekend trying to understand why ‘Covid19 mortality rate’ in e.g. Lombardy seems to be way higher compared to Germany. Then I started to realize how data is used here and since then I can only wonder. That’s why I mentioned data literacy being the main problem.
>Which data is backing this? Surveys where testing not just focused on ‘sick’ or dead people in hospitals but also included asymptotic people (so going towards a representative sample) ‘found that 50% of all test-positive persons showed „no symptoms“ at all, while the other 50% mostly showed „very moderate cold-like symptoms“.
interesting.. if you then cite a blog which cites buzz feed (buzzfeed dot com/albertonardelli/coronavirus-testing-iceland) which cites some other weird cites from the things tests happening in Iceland where you’ve (according to buzz feed cause I’m honestly too lazy to go down the whole rabbit hole of these crappy source citing other crappy source sites to see where those data comes) tested 3300 people with 218 positives.. A nightmare for everyone doing serious data analysis.. the perfect data set to back whatever opinion you have with some random numbers. So if we go into this data a bit further (we still stay on buzz feed no worry), the data set splits up into this statement (1):
>”At least half of those infected contracted the virus while traveling abroad, mostly in high-risk areas in the European Alps (at least 90),” the government said on Monday.
and (2):
>Those numbers include the first results of the voluntary tests on people with no symptoms, which started last Friday. The first batch of 1,800 tests produced 19 positive cases, or about 1% of the sample.
and the one where your statement comes from(3):
>”Early results from deCode Genetics indicate that a low proportion of the general population has contracted the virus and that about half of those who tested positive are non-symptomatic,” said Guðnason. “The other half displays very moderate cold-like symptoms.”
and finally (4):
“This data can also become a valuable resource for scientific studies of the virus in the future,” he added.
1: well that’s what you see in every virus spreading emulation.. the first one comes from a hotspot and then spreads..
2: the random part of those ‘data’ is testing 1800 out fo 3300 with 19 positives with no symptoms
3: No idea how he comes to that conclusion.. we’ve the number of 19 positives with no symptoms and the other 199 positives with no description of how they’re doing.. after in all it’s not a scientific paper it’s just some sort of an interview done by journalists which wrote articles like:
“4 Things Boris Johnson Said About Brexit At Prime Minister’s Questions That Weren’t Really True”
(Emily Ashton) and
“These Are All The “Dear Donald” Letters Theresa May And Boris Johnson Sent Tusk Since The Brexit Referendum” (Alberto Nardelli)
Not that I think they’re bad journalists but I don’t think they’re good enough to question or ask an epidemiologist the right questions..
4: nobody ever in science will tell you that the data he collects is worthless..
what we IMO have is interpretation of noise of a virus spreading before exponential grow phase with a population which neither represents europe or asia or US with a laughable sample size and an opinion from their chief epidemiologist. Or… the average BS you read in news when it comes to science.. Cause we neither understand statistics nor the exponential growth rate nor incubation time..
>So why do we treat a positive test result as illness? It might be just an infection but the tests used seem to have a high false-positive rate anyway.
do we? and where? And for the second part.. there’s not one single test used.. and I didn’t saw any data which backs your claim about the hight false-positive rate. What we currently mostly see in testing is PCR tests for two parts of the virus RNA with roughly 100-120 bases. A test which looks ‘at a first glance’ pretty much generic and I wouldn’t expect much more false positives/negatives as with every other PCR test.. except it’s RNA based one and it seems that sample collection isn’t that easy so we would expect more false negatives due to wrong sample handling, collection and if labs are overloaded maybe wrong sample workup (before you can do PCR you’ve to extract the RNA and this step is prone to fail.. whereas a fail will give you likely a false negative – at least when you do manual testing.. I’ve no personal experience in the devices hospital labs use). PCR amplification of RNA can only be done when enough virus RNA is available from the sample means during an active infection. I didn’t found an article worth to cite about robustness of those tests and when during an infection the test will give you a positive results (to figure out when testing makes sense). It might be that the virus can be detected before symptoms show up.. I don’t know.. I guess we’ll have already studies out somewhere which took a look at those tests.. But I wouldn’t make a claim about that till I’ve seen proper data.
The second set of tests is based on antibodies (e.g. everything called ELISA test). Those are rather new available in a broader scope (synthesize the primers for PCR to produce ‘covid 19’ PCR kits is something a bunch of labs can once the sequences are out and the scientific community tends to share that stuff quite open: https://www.ncbi.nlm.nih.gov/genbank/sars-cov-2-seqs/ whereas producing antibodies for those tests is rather complicated they need a longer ‘ramp up’ time in production. and you need to validate them). Antibody test are interesting cause you can monitor for antibodies which should stay after the virus isn’t detectable by PCR anymore and testkits for ‘low tier’ labs can be developed easy (e.g. the common pregnancy test you can buy in the super marked is an ELISA based antibody test). Once we have those antibody tests in quantities high enough to test random people we might be able to estimate how wide it spreads, how many go ‘asymptotic’ and how much of an issue the whole thing is. We simply don’t have the testing capacity needed yet.
@willy for “We should aim at seeing the virus spread as fast as hospitals can reasonably deal with”
speaking of france, alsace is already over the acceptable number, they send patients to switzerland cause they run out of space for those needing respiratory support. The thing with exponential growth is.. if you do a minor mistake in your assumptions, the impact might be big.
For those interested in leaving the buzzfeed world and going into more trustworthy data:
http://www.neotropicalscience.com/uploads/4/6/7/6/46762515/covid-19.pdf
table 1 is worth to read.. actually the whole paper is.. For those thinking that their country does better than italy.. let’s discuss this in 10-12 days that’s what I assume (or let’s be honest here it’s more a guess) italy is ahead of most of us here in europe, once hospitals look like this one https://www.youtube.com/watch?v=y39Y6ANewME we’ll see if this is only a ‘local effect’ or if europes health care system at all isn’t capable to deal with it..
> For those thinking that their country does better than italy.. let’s discuss this in 10-12 days
Sure.
In the meantime studying lists of facts instead of sensational media reports resulting in trillions of people panicking seems a good idea to me: https://swprs.org/a-swiss-doctor-on-covid-19/
BTW what went wrong in Italy is nicely explained here: https://www.youtube.com/watch?v=JNFVJIFGGs0
In France, doctors say they have almost no more report of heart or brain attacks, nor prostatis cancers. How many such undiagnosed people will die early due to the *measures* in place instead of the virus ? There’s no need to prevent people from going out if the problem is just to prevent them from being close to each other. However by packing many of them in an appartment, you’re certain to spread the virus from one person to all inhabitants. And in general there’s no way a frozen country will efficiently fight any attack, including a virus. You need all forces to stay active to develop masks or medicines. For example one of the reasons we’re missing doctors is that many are forced to stay home to keep their kids! And that’s true in many activities. Truck drivers don’t want to work anymore because restaurants/hotels are closed and they need to have a place to eat/wash/sleep. This directly impacts the time to ship food and masks!
How is that comparable? Hong Kong has 75% of Sweden’s population in 1/450th the area.
> How is that comparable? Hong Kong has 75% of Sweden’s population in 1/450th the area.
No idea how that’s comparable or why you compare?
I mentioned Sweden as an example of an European country that did not turned from a democracy into a totalitarian police state within the last weeks unlike many others.
And Sweden seems to deal pretty well with this pandemic based on the data published. All without police, the military, mass surveillance and locking down the whole country. They simply try to protect those who need to be protected and tell ill people to stay at home to not further spread this virus (or all the other viruses nobody is testing for currently).
Wrt wearing masks as common in Asia… I think it’s a great idea doing this during the yearly Flu season to protect others from oneself spreading viruses and bacteria. Needs to be adopted by everyone then of course. And I’m not talking about N95 or FFP masks. 🙂
Well in France it’s simple: you can’t go to work, you’re forced to stay home, you can’t go out without signing a duly dated and filled authorization, and you can’t even do your errands because they organize endless queues in front of supermarkets in which they only let 10 people in every 20 minutes! So basically I eat bad food that I refill once a week from a local store that’s still accessible. And with the absurd measures that were taken here now they’re scared to put an end to the confinement because likely too few people were infected and the population is not immune. Surprizing! They managed to totally scare the whole population for something that affects much less than 1% of it, yet people applaud every evening on their balconies. And people are so much scared that now they want to stay confined! I’d say “kudos” to the governments who for the first time in humanity history managed to enjail 3 billion people by scaring them of something they can’t see, benefitting from the complicity from media and stupid rumors on social networks making it appear worse than it really is! They’d have already saved more 10x more lives by stopping alcohol or tobacco sales!
It’s pretty conceivable that tobacco/nicotine liquids will be next, partly out of geniune humanistic ideas, partly out of the desire for more control.
In quite a lot of developed and developing countries smoking is already stigmatized in media and confined to designated areas in real life. Given the overall level of fear, it would be a waste of a perfectly good crisis to not to point at smokers and say: “Hey, they’re deliberately making themselves an easier target for the virus for their egotistic pleasure! They will be a liability when the next wave comes! Either they’re addicted and we must treat them, either they’re irresponsible and we must educate them, either they are malicious and we must punish them.”
I’d say smoking will be even more priced out out of the reach of an average citizen with additional “social responsibility” sale taxes on nicotine products that ostensibly will go to fund hospitals (new objects of worship) and it probably will be lauded on from the balconies. Expensive smoking like good cigars will come up in price, but not that much relatively.
That’s a low-hanging fruit, alcohol still stands a bit too strong to attack it head-on, but after the tobacco is dealt with, alcohol will be easier.
Fun times.
The sale of alcohol is banned for two weeks in some provinces in Thailand to prevent people from socializing.
Lets not forget many people are trying to win Darwin Awards, even if their not aware they are doing so.
Darwin Awards: Vote for the Award Nominees! The Darwin Awards commemorate the (remains of) individuals who contribute to the improvement of our gene pool by removing themselves from it.
> they’ve literally stopped the virus in Taiwan Korea and China
Nobody knows how the virus spreads in either country. It’s just that they do not report as much positive test results as in the past (which can simply be the result of less testing). To know how the virus spreads you need to test against a representative mix of the population and not just on ‘patients with symptoms’ or ‘contact persons’. Same problem with ‘Covid19 deaths’ and then the calculated ‘death rate’ by using these two numbers.
The 1st number is way under-estimated and the 2nd largely over-estimated (since we count deaths with Covid19 as deaths due to Covid19 which is obviously wrong). We need to look closer at the data available and how it’s used: https://www.spectator.co.uk/article/how-to-understand-and-report-figures-for-covid-19-deaths-
fun part is that in .pl we dont count 2nd AT ALL. a lot of deaths are classified as co-existing diseases, which gives false results. also, the main reason to slow down the initial spread, is to allow hospitals and other services to still work during the pandemy.
> fun part is that in .pl we dont count 2nd AT ALL
And the 1st number which should indicate how the virus spreads is obviously a misinterpretation since as in every other country the data collected is not from a representative sample. We’re treating persons with a positive virus test as ‘Covid19 patients‘ which is already strange and then we take these numbers as an indication how the virus would spread within the population.
In germany we see an exponential growth in test-positive persons (called ‘Covid19 patients’ even if not showing any symptoms at all) obviously due to an exponential growth in tests done (while the relative positive rate stays rather identical): https://swprs.files.wordpress.com/2020/03/anzahl-infizierte-und-tests-2603.jpg
What do these numbers show when interpreted carefully? An increase in Covid19 infections? No, just an increase in tests done while showing a constant test-positive rate (quite the opposite one would expect if there is a virus outbreak going on).
What if the virus already spread and infected large parts of the population? This can only be answered by a test done with a representative sample. And maybe a test should be used that shows a false-positive rate for asymptotic people not close to coin flipping…
You could say that, but then, the death toll is also going up exponentially, and that invalidates your statement.
And if you doubt the death toll being attributed to covid-19, up to this day, up to this time, I know only of 3 studies that confront covid-19 attributed deaths with variations in the normal death rates expected. (1 for Spain, 1 for a few Italian regions and another for my country.
The numbers don’t match: Increases in the number of deaths in relation to expected numbers are about 4x the numbers being reported for covid-19.
The Portuguese government has initiated a formal investigation into the issue today.
This is FUD. Yes there is some ambiguity in case numbers and you can’t make a definitive numerical assessment with valid error bounds. And yes, I agree that estimates of the death rate are very fuzzy, but it’s the best we have and in the end it’s hardly relevant from a policy standpoint. The death rate in countries that handled the situation poorly (like Italy), whatever it is, is clearly problematic and given the chaos you see currently in hospital systems I think you’d agree it’s at the very least much higher than the standard flu. It’s well beyond what we as a society would consider acceptable. The final death-rate number is not longer relevant
Furthermore, just because the numbers aren’t ideal doesn’t mean there is some hidden wave of sick people (which you seem to suggest in your other reply). This is just obvious at face value b/c hospitals in Korea Hong-Kong Taiwan aren’t being slammed like there are in the West. And there hasn’t been some secret asymptomatic inoculation of the populations b/c for instance Taiwan never even had a full pandemic stage (they close their borders very early) and the country as a whole has had very few cases in total. So unless bubble-tea magically suppresses the symptoms of COVID-19, people here clearly have not been exposes to the virus. The travel restrictions and self-quarantining measures have just demonstrably worked. Questioning the statistics of the numbers is fine, but saying the policies haven’t worked is just ignoring the realities of the on-the-ground impact of different policy decision. Life in Taipei has been normal b/c they took it serious. Life in Europe is not b/c half the people are at home and half the people are saying it’s impossible and doing mental gymnastics to justify it for themselves. This FUD people keep spreading is doing a lot of harm b/c it’s making the situation out to be unsolvable when we has specific counterexamples
> This FUD people keep spreading is doing a lot of harm b/c it’s making the situation out to be unsolvable when we has specific counterexamples
Not being able to feed and heal correctly 100% of a country while around 0.05% passed through hospitals is not FUD but a reality. I’ve been eating shit food for 3 weeks now and will soon really need to find a dentist. And I’m not the only one, it’s the same for 100% of the country.
And regarding hospitals, even if medical staff really suffers from the situation, it’s important to note that we’ve had 12k people leave hospitals healed for 4k deaths without having to give up on some of them, an ~15k still under treatment (up to ~3 weeks). This means that we’re able to handle roughly 20k people/month knowing among them we’ll lose 6k regardless of the number of places. Above 20k/mo we’d lose 100% of extras by lack of treatment instead of only 25%. It’s worth noting that in this country we already lose 820k people/yr, which is more than estimates of what the virus can cause to 100% of the population, and this will increase by lack of treatment of diseases, infections, brain/heart attacks, suicide attempts or home accidents.
Worse, some people who got scared by this disease are getting totally mad at anyone else and are developing hate against doctors living in their building, trying to force them to move away by fear of being infected! We’re ruining the society and developing a huge amount of violence and hate which will have other effects not yet accounted for.
The real FUD here is that the virus is the problem. The reality is that the measures taken against it are the real problem. Keep in mind that with 20k people treated for 67M people, it has touched so few people that the major part of the population doesn’t even know someone who knows someone who had to be treated for it!
That’s not FUD but just simple numbers any kid can understand.
The masks protect others from you, not you from others. They do not protect you from inhaling aerosolised droplets from someone coughing or sneezing. They do provide a small amount of protection for others near you if you cough or sneeze and you are a carrier.
If you are healthy, wearing the mask is a waste of resources, and a false sense of security.
Wearing a mask when you are healthy just sends the wrong message, to yourself and to the vastly ignorant general population around you.
“They do not protect you from inhaling aerosolised droplets”.
They also don’t protect me from falling pianos. That’s not the point.
“If you are healthy, wearing the mask is a waste of resources, and a false sense of security.”
Do people do daily tests? How would anybody know their aren’t infected and contagious?
Testimony from people wearing face masks and protective eyewear also go against your statement about them giving a false sense of security. People who actually use them mostly say they act as a constant reminder that the situation isn’t normal, and that extra care should be taken.
They also help to protect against everyday gestures that are difficult to avoid, like people frequently touching their faces and eyes.
Furthermore:
1 – The numbers coming out from countries that require face masks vs the ones who discourage them, say you’re wrong.
2- The experts in countries that had to fight MERS and SARS say you’re wrong.
As a side note, a few days ago, the head of the Portuguese health organization coordinating the crisis actually said that the reason they don’t recommend general usage of masks is because they don’t have enough of them even for the the health staff.
That I can actually accept (as their recomendation). Lying about it is a different thing.
Everybody is a expert back seat driver suddenly. Hindsight is 20:20 vision.
” Should more of us wear face masks to help slow the spread of coronavirus?
This question is to be assessed by a panel of advisers to the World Health Organization (WHO).
The group will weigh up research on whether the virus can be projected further than previously thought; a study in the US suggests coughs can reach 6m and sneezes up to 8m.
The panel’s chair, Prof David Heymann, told BBC News that the new research may lead to a shift in advice about masks.
The former director at the WHO explained: “The WHO is opening up its discussion again looking at the new evidence to see whether or not there should be a change in the way it’s recommending masks should be used.” ”
bbc.co.uk
” Covid-19 3d printable mask approved – only for MJF printers, files available
The Czech Republic has certified a 3D printed anti-covid-19 mask, as a half-mask with FFP3 safety level to EN 140:1999 when using exchangeable external filters. ”
electronicsweekly
When things get bad enough, people in charge feel they have to lie to the public to avoid panic, and make things worse, as would be the case for bank runs for instance.
Jean-Claude Juncker, President of the European Commission at the time, famously said ‘When it becomes serious, you have to lie”.
So people have to find out what’s right by themselves…
Agreed, which is why with our government saying “we’ll be transparent” it’s not that serious 🙂
I see a lot of bushfire experts changed their area of expertise to epidemiology in a matter of months.
It’s uplifting: with millions of fluid experts debating the truth on the global marketplace of ideas humanity is sure to overcome anything and we may even achieve cold fusion (in twenty years, as customary).
Ultimately in the long haul a lot will be defined by the containment measures enforced by different governments we live under jurisdictions of.
That’s another very intersting topic to discuss with all-around experts, especially when and if these sweeping powers will be ratcheted down.
Regarding personal protection measures, over the ear masks seem to be better than nothing.
Masks introduce rituals. A mask (over the face or on chin, at the ready) is a constant reminder that things aren’t normal, think twice before doing things. A mask puts quite a weight on your personal integrity (no, I can’t smoke at the street, I’m in a mask, that’d be hypocrisy). A mask is excellent at making kids not put their fingers into mouth and if you enforce them wearing a mask, you have to wear one yourself. At places where (and when) masks are yet not common, you’re looked at as a freak or doomsday prepper and avoided.
That’s assuming you’re maximizing delaying infection as long as possible, hoping for a vaccine or better treatment (malaria drugs are pretty heavy-handed, I heard).
As the information on the antibodies is not that conclusive and as slowly drowning is an especially nasty way to go, that seems to me like a nice metric to optimize for.
Sorry, but this situation isn’t great. I got some masks, because I do soldering work. But not these kind of masks. If I would get my hands on these masks, I would rather donate it to a local hospital than using it myself. This is ridiculous. Now, we are giving face masks to people with good connections? Not happy about it…
People who get it can still donate it if they want. However, from the post on Pine64 and other sources I’ve read, I understand medical professionals really need N95 masks for optimal protection, and not the type of surgical mask Pine64 is giving away.
FFP3 are even better. But currently, if they have the option between surgical masks or no masks, they probably choose the surgical ones. And that is the point here. And this is what I don’t like.
Tkaiser is right. There is no excuse to implement a totalitarian state. The knee jerk reaction will kill and ruin far more than the virus. Poor people and businesses are being destroyed. Supply chains are ripped to shreds which will have far more deadly impacts that will only be evident a month from now. People just do not think ahead and realize the complexities. You cannot base policy on a one-dimensional metric that is not uniform or even consistently measured. Healthcare overrun must be on the table as an acceptable end in order to prevent other even more catastrophic ends.
This morning on the radio a professor working in a hospital said that estimates are that in France the confinement has saved around 2500 lives to covid-19 but will likely have killed many more from various other causes, first ones being worse hygiene and lack of medical treatments for various other things. That’s exactly what I’ve been suspecting would happen from the beginning. The worst is that we’re now “discovering” that it worked too well here and that possibly too few people have been infected yet to relax the rules…
Also I can’t stand anymore all these selfish people thinking “let’s go on like this, my life is still OK with confinement”, without thinking about all the people ruining their own lives and taking all the risks in order to bring them their food, electricity, networking, water, security, medical care and whatever they need to keep a cool life!
Same for those who say “you see it’s easy to stop polluting”. The reality is that this situation cannot stand long, the world is just surviving on its accumulated reserves and everyone is still consuming far more than we’re producing. We’re just running in front of a wall and it seems some are too blind to see it.